
Saliva is the most accessible human biofluid for cytokine monitoring — requiring no venipuncture, no specialised clinical staff, and minimal participant discomfort. These advantages have driven its adoption in paediatric immunology, stress research, oral microbiome studies, and large-cohort epidemiological screening.
However, saliva presents unique analytical challenges: cytokine concentrations are typically 10- to 100-fold lower than in serum, collection method dramatically affects measured concentrations, and the biological signal in saliva predominantly reflects local mucosal immunity rather than systemic immune status. This guide covers what can and cannot be detected by Luminex in saliva, which collection methods preserve cytokine integrity, how to process samples correctly, and when saliva is the appropriate matrix choice.
What Luminex Can and Cannot Detect in Saliva
Instrument capability
All three major Luminex reader platforms — Luminex 200, MAGPIX, and FLEXMAP 3D — can process saliva samples. The detection sensitivity difference between these instruments for saliva applications is minimal; the limiting factor is the biological concentration of cytokines in saliva, not the instrument's photon detection capability. The LX200 and FLEXMAP 3D use dual-laser detection; the MAGPIX uses LED-based detection with slightly lower sensitivity for the lowest-concentration analytes but remains sufficient for IL-1β, IL-6, IL-8, and TNF-α in most saliva samples.
Analyte detectability
Data from published validation studies comparing saliva and serum cytokine concentrations by Luminex (Schmidt et al., 2026):
| Cytokine | Saliva Range (pg/mL) | Serum Range (pg/mL) | Saliva/Serum Ratio | Quantifiable by Standard Luminex? |
|---|---|---|---|---|
| IL-1β | 10–200 | 5–50 | ~2–4× | Yes — often higher in saliva |
| IL-1α | 50–500 | ≤5 | ~10–100× | Yes — constitutively expressed in oral epithelium |
| IL-6 | 1–50 | 5–100 | ~0.1–0.5× | Detectable in most samples |
| IL-8 (CXCL8) | 10–300 | 5–50 | ~2–6× | Yes — abundant in saliva |
| TNF-α | 1–30 | 10–100 | ~0.1–0.3× | Borderline — near LLOQ in healthy individuals |
| IFN-γ | ≤10 | 10–500 | ~0.01–0.02× | No — below LLOQ in most samples |
| IL-2, IL-4, IL-10, IL-12 | ≤1–5 | 5–500 | ~0.001–0.01× | No — below detection floor |
The pattern is consistent: inflammatory markers produced locally in the oral cavity (IL-1β, IL-1α, IL-8) are readily detectable, while T-cell-derived cytokines (IFN-γ, IL-2, IL-4, IL-10, IL-12) are generally below standard Luminex detection limits in saliva. For ultra-sensitive detection of low-abundance cytokines, see our Simoa digital ELISA service.
Saliva Collection: Method Matters More Than Most Researchers Realise
| Method | Cytokine Recovery (vs Passive Drool) | Mechanism of Loss |
|---|---|---|
| Passive drool | 100% (reference) | None — direct collection into tube |
| Salivette (cotton swab) | 60–80% | Cotton fibres adsorb IL-1β, IL-6, IL-8, TNF-α; recovery varies per analyte |
| Stimulated saliva (citric acid/paraffin) | 40–60% | Increased flow rate dilutes cytokines; stimulant may alter local immune status |
Passive drool is the standard: participant tilts head forward, allows saliva to pool for 1–2 minutes, drains through a short straw directly into a pre-chilled tube kept on ice. Typical yield: 1–3 mL over 3–5 minutes. If Salivette must be used for clinical workflow reasons, polyester swabs (not cotton) and pilot validation of recovery rates per analyte are the minimum standard.
Circadian and dietary effects
Salivary cytokine concentrations are not static across the day. IL-6 and TNF-α show a diurnal pattern with peak levels in the early morning (06:00–08:00) and a nadir in the late afternoon, with intra-individual variation of 20–40% across timepoints (Riis et al., 2015). For longitudinal studies, collecting all samples within a 1–2 hour window across all visits reduces circadian confounders to the level of assay variability.
Dietary intake also introduces acute effects. Standardising collection to the morning fasting state — before eating, drinking, toothbrushing, or smoking — eliminates these confounders. If fasting collection is not feasible, a minimum 60-minute abstinence from food and drink (water excepted) before collection is the commonly accepted compromise.
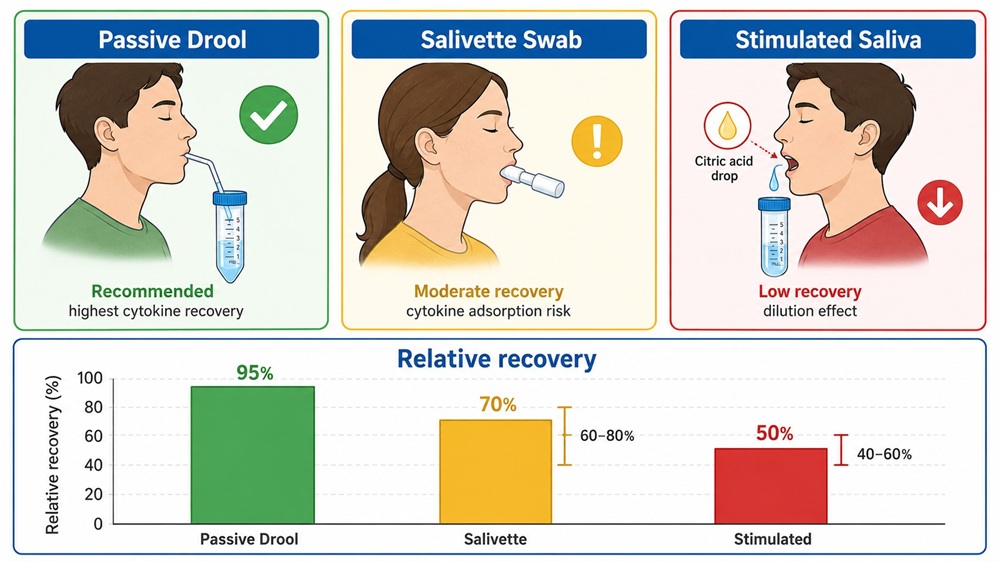 Saliva collection methods and their effect on cytokine recovery: passive drool yields the highest and most reproducible concentrations, while cotton Salivette and stimulated methods introduce analyte-specific losses of 20–60%.
Saliva collection methods and their effect on cytokine recovery: passive drool yields the highest and most reproducible concentrations, while cotton Salivette and stimulated methods introduce analyte-specific losses of 20–60%.
Sample Processing: The Difference Between Data and Noise
- Timing: Centrifuge within 30 min of collection. If not possible, place on wet ice immediately and process within 2 hours.
- Centrifugation: 10,000–14,000 × g, 10–15 min, 4°C. Transfer clear supernatant, avoiding the pellet of mucin, cells, and bacteria.
- Protease inhibitors: Add aprotinin (1–2 µg/mL), PMSF (0.1–1 mM), leupeptin (1–10 µg/mL). Saliva contains active proteases that degrade IL-1β and IL-6 within hours at room temperature.
- Aliquoting: Single-use aliquots of 75–100 µL (25 µL per Luminex well × 2–3 replicates). Label with sample ID, date, and freeze-thaw count.
- Storage: Snap-freeze in liquid nitrogen or dry ice-ethanol bath, then transfer to −80°C. At −80°C, samples are stable for ≥12 months. At −20°C, degradation is measurable within 2–4 weeks.
- Shipping: Dry ice, insulated container with temperature logger. Do not ship on wet ice — incomplete freezing causes partial thaw-refreeze.
What degrades salivary cytokines
- Freeze-thaw cycles: Each cycle reduces IL-6 and TNF-α by 10–20%. After 3 cycles, concentrations may be 30–50% lower. Single-use aliquots are the definitive prevention.
- Room temperature: IL-1β declines ~5% per hour at 25°C in unprocessed saliva.
- Vortexing: Re-suspends debris, introduces bubbles. Pipette gently instead.
When Saliva Is — and Is Not — the Right Matrix
Appropriate applications
- Oral and periodontal disease: Salivary IL-1β, IL-6, IL-8, TNF-α correlate with clinical severity indices.
- Upper respiratory infection: Salivary IL-6, IL-8 increase during influenza, SARS-CoV-2, and bacterial pneumonia.
- Oral microbiome–immune interaction: Single sample for paired metagenomic and cytokine profiling.
- Paediatric and elderly populations: Non-invasive longitudinal sampling.
- Stress and psychoneuroimmunology: Salivary cortisol-cytokine axis well-characterised.
- Exercise immunology: Repeated sampling across training sessions to monitor mucosal immune status.
When saliva is not appropriate
- Systemic inflammatory disease monitoring: Does not reliably track serum IL-6, CRP, or IFN-γ in RA, SLE, or sepsis. Serum or plasma required.
- T-cell cytokine profiling: IL-2, IL-4, IL-10, IL-12, IL-13, IL-17A, IFN-γ are below standard Luminex detection in saliva.
- Pharmacodynamic studies: Intra-individual CV 30–50% vs 15–25% for serum — unsuitable for PK/PD modelling.
- Cross-study comparisons without method standardisation: Passive drool IL-6 cannot be compared to Salivette IL-6.
For studies requiring both systemic and mucosal data, a two-matrix design — serum for systemic markers and saliva for mucosal markers — provides complementary insight. Explore our Luminex cytokine detection service for customised panel design across matrices.
Practical Study Checklist
- Confirm analyte detectability: Cross-reference targets with the table above before committing to saliva.
- Standardise collection: Passive drool, same time of day (morning, before eating/drinking/toothbrushing), all participants, all timepoints.
- Document oral health: Record gingival bleeding, recent dental work, lesions, medications (NSAIDs, steroids) at every visit.
- Process within 30 min: Centrifuge, add protease inhibitors, aliquot, snap-freeze, store at −80°C.
- Include pooled saliva QC: Pool from 5–10 representative samples; run on every plate; monitor %CV (target ≤ 20%).
- Plan LLOQ strategy before collection: Pre-specify how
References:
- Schmidt, S., et al. "Comparative study of cytokine measurements in blood plasma and serum and saliva using a multiplexed bead-based assay." Veterinary Sciences 13(1) (2026): 68. DOI: 10.3390/vetsci13010068
- Williamson, S., et al. "Comparison of biomarkers in blood and saliva in healthy adults." Nursing Research and Practice (2012): 246178. DOI: 10.1155/2012/246178
- Riis, J. L., et al. "Salivary cytokines as a minimally-invasive measure of immune functioning in young children." Developmental Psychobiology 57(6) (2015): 699–710. DOI: 10.1002/dev.21324
- Granger, D. A., et al. "Integration of salivary biomarkers into developmental and behaviorally-oriented research." Physiology & Behavior 92(4) (2007): 583–590. DOI: 10.1016/j.physbeh.2007.04.004
- Navazesh, M. "Methods for collecting saliva." Annals of the New York Academy of Sciences 694 (1993): 72–77. DOI: 10.1111/j.1749-6632.1993.tb18343.x