
Introduction to Inflammation Biomarkers in Cardiovascular Disease
Inflammation shapes every stage of atherosclerosis—from endothelial activation and monocyte recruitment to plaque progression and vulnerability. For research-use only (RUO) studies in cardiovascular disease, inflammation biomarkers help investigators map pathways, stratify cohorts, and monitor responses in longitudinal designs without making diagnostic claims. Among the most informative analytes are interleukin-1 (IL-1, especially IL-1β), interleukin-6 (IL-6), interleukin-18 (IL-18), tumor necrosis factor alpha (TNF-α), and C-reactive protein (CRP). Together, they cover three complementary axes: an inflammasome pathway (IL-1β and IL-18), a systemic acute-phase cascade (IL-6 → CRP), and an endothelial activation link (TNF-α).
Use this guide to decide when to use which biomarker in chronic atherosclerosis progression and plaque vulnerability research. The primary lens is practical: panel composition, matrix choice (serum vs plasma), assay modality (multiplex vs singleplex), and fit-for-purpose validation. Throughout, we'll keep the focus on inflammation biomarkers in cardiovascular research and avoid any diagnostic framing.
When to Use IL-1, IL-6, IL-18, TNF-α, and CRP in Cardiovascular Research
IL-1: Role and Use Cases in Research
IL-1β is produced via NLRP3 inflammasome activation and amplifies local vascular inflammation, contributing to plaque progression and instability. As an upstream node, it connects mechanistic findings to downstream systemic signals.
- Role: Inflammasome-driven cytokine shaping plaque biology; links to the IL-6–CRP systemic axis. Recent reviews outline how NLRP3 priming and caspase‑1 maturation fuel IL‑1β in vascular beds, influencing instability phenotypes, as summarized in the 2023 overview on inflammasomes in atherosclerosis in the journal Cardiovascular Research.
- When to use: Mechanistic atherosclerosis studies, plaque vulnerability models, and upstream intervention hypotheses.
- Practical notes: Low circulating levels demand sensitive methods and tight pre-analytical control—plasma (EDTA) often preferred to limit ex vivo release; confirm near-LOD signals with singleplex where possible.
- Long-tail fit: IL-1 beta inflammasome cardiovascular research.
IL-6: Role and Use Cases in Research
IL-6 is a central node in the systemic inflammatory response, inducing hepatic CRP and tracking disease activity across atherosclerosis and heart failure research.
- Role: Acute-phase driver and integrator of vascular inflammation. Large-scale syntheses show IL‑6 associates with adverse outcomes and progression in cardio‑cerebrovascular settings; for example, a 2021 meta‑analysis in Frontiers in Cardiovascular Medicine linked IL‑6 with ACS severity, and newer individual‑participant analyses (2024–2025) reinforced risk associations in longitudinal cohorts.
- When to use: Longitudinal progression and risk-enrichment studies; therapy-response monitoring; bridging local vascular events and systemic readouts.
- Practical notes: Robust in both serum and plasma when SOPs control for processing time; combine with CRP to represent the IL-6 CRP axis in atherosclerosis studies.
- Long-tail fit: IL-6 CRP axis in atherosclerosis studies.
IL-18: Role and Use Cases in Research
IL-18, processed by inflammasomes, frequently travels with IL-1β as a co-signal of plaque inflammation and potential vulnerability.
- Role: Pro-inflammatory cytokine associated with atherosclerotic plaque burden and adverse features. In a 2024 imaging-linked study, higher IL‑18 and IL‑18/TRAIL ratios correlated with greater CTCA-quantified atherosclerosis burden and adverse plaque characteristics.
- When to use: Chronic progression and vulnerability studies; pair with IL-1β to quantify inflammasome activity; consider ratio metrics (e.g., IL-18/TRAIL) alongside imaging-defined endpoints.
- Practical notes: Often low abundance; leverage multiplex discovery and confirm with ultrasensitive singleplex if values cluster near LOD.
- Long-tail fit: IL-18 plaque vulnerability biomarker.
TNF-α: Role and Use Cases in Research
TNF-α is a macrophage-derived cytokine that promotes endothelial activation and atherogenesis via NF-κB/MAPK signaling, elevating adhesion molecules and vascular permeability.
- Role: Connects macrophage-driven inflammation to endothelial dysfunction and lesion progression. Reviews highlight its role in upregulating ICAM‑1/VCAM‑1 and promoting monocyte adhesion and foam cell formation.
- When to use: Studies exploring disease progression and links between systemic inflammation and endothelial activation; adjunct to IL-6 in progression profiling.
- Practical notes: Moderate abundance but context dependent; interpret with endothelial readouts (e.g., adhesion molecules) when available.
- Long-tail fit: TNF-alpha endothelial activation inflammation.
CRP: Role and Use Cases in Research
CRP is a downstream acute-phase reactant induced by IL-6, providing a robust measure of systemic inflammation over time.
- Role: Established systemic marker for risk tracking in cardiovascular cohorts, frequently used to complement IL‑6 for a fuller view of systemic inflammatory load.
- When to use: Longitudinal monitoring and cohort enrichment; pair with IL-6 for systemic axis coverage.
- Practical notes: Typically higher concentration and analytically tractable; singleplex hs-CRP assays are standard for confirmation and cross-study comparability.
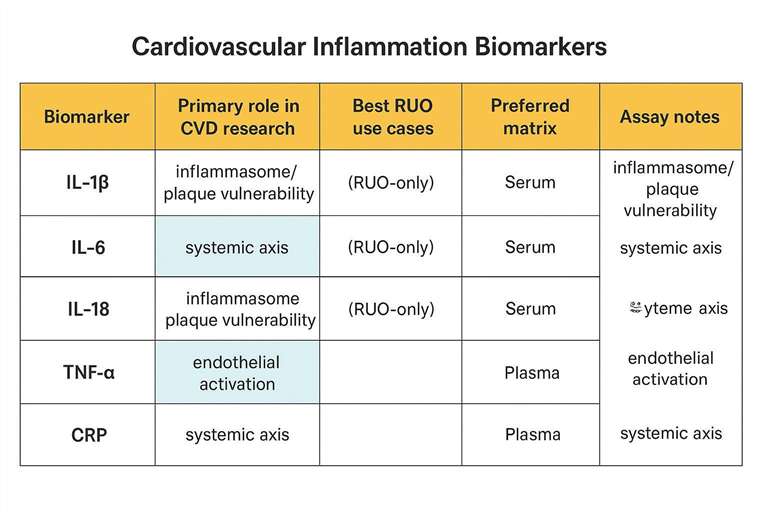 A table comparing IL-1β, IL-6, IL-18, TNF-α, and CRP with their roles in cardiovascular disease research.
A table comparing IL-1β, IL-6, IL-18, TNF-α, and CRP with their roles in cardiovascular disease research.
Choosing the Right Inflammation Biomarkers in Cardiovascular Research
Selecting Biomarkers Based on Research Focus
Acute windows call for IL‑6 and TNF‑α to profile short-lived inflammatory surges, such as around ACS or procedural stress. For chronic conditions, CRP and IL‑18 help monitor atherosclerosis progression and vulnerability phenotypes over longer horizons; pairing IL‑1β with IL‑18 strengthens the mechanistic readout of inflammasome activity.
Choosing the Best Biomarker for Risk Assessment Studies
For long-term risk, IL‑6 and CRP form a complementary systemic axis well-suited to cohort enrichment and longitudinal tracking. For pathway insight, IL‑1β and TNF‑α help dissect inflammation-related mechanisms, with IL‑18 signaling inflammasome-linked vulnerability—especially when integrated with imaging or endothelial readouts.
Factors to Consider in Biomarker Selection
Sensitivity and specificity requirements should match expected concentration ranges, particularly for IL‑1β and IL‑18 near assay LODs. Start broad with multiplex in discovery, then confirm key findings with singleplex for standardization. Balance panel breadth with throughput, sample volume, and QC overhead.
Case 1: Plaque vulnerability and inflammasome activity mapping
Study goal: Stratify plaque vulnerability phenotypes and test inflammasome-linked hypotheses without diagnostic claims.
Suggested marker set (one-run discovery panel): IL‑1β + IL‑18 (inflammasome axis) + IL‑6 + CRP (systemic acute-phase axis) + TNF‑α (endothelial activation linkage). If imaging is available, prespecify how biomarkers will be integrated with CTCA/CTA plaque features (e.g., low-attenuation plaque, positive remodeling) rather than interpreted as standalone readouts.
Matrix & handling: Prefer EDTA plasma for low-abundance IL‑1β/IL‑18 to reduce ex vivo release; standardize time-to-spin (target ≤4 hours), aliquoting, and freeze–thaw limits across all visits.
Assay strategy: Use multiplex for discovery/phenotyping, then confirm near-LOD IL‑1β/IL‑18 signals with a higher-sensitivity singleplex method where feasible; keep CRP on a standardized singleplex (hs‑CRP) if cross-study comparability is a priority.
Analysis notes: Predefine rules for <LOD values (left-censoring or prespecified imputation), and interpret results as pathway-aligned patterns (IL‑1β/IL‑18 together; IL‑6/CRP together) rather than isolated p-values.
Case 2: Longitudinal cohort monitoring (systemic axis)
Study goal: Track inflammation dynamics over months/years and relate within-subject changes to progression endpoints (RUO).
Suggested marker set (core + optional): Core = IL‑6 + CRP to represent the systemic axis; optional add-on = TNF‑α when you also collect endothelial activation readouts or want a macrophage–endothelial linkage signal. Add IL‑1β/IL‑18 only if the study question explicitly tests inflammasome biology (because they are more frequently near LOD in circulation).
Matrix & assay consistency: Lock matrix (serum or plasma) and anticoagulant up front and do not switch mid-study. For multi-batch studies, include the same QC materials (high/low controls) on every plate/run and document kit lot numbers.
QC & reporting: Report LOD/LOQ and intra-/inter-assay %CV; prespecify how you will handle values <LOD; avoid comparing absolute concentrations across platforms unless you have a bridging/normalization plan.
Interpretation: Emphasize within-subject deltas and trajectory patterns (e.g., sustained elevation vs transient spikes) rather than single time-point comparisons.
Tools for Measuring Inflammatory Biomarkers
Multiplex Assays for Inflammation Biomarkers
Multiplex platforms allow simultaneous quantification of multiple analytes with small volumes—ideal for linking inflammasome, systemic, and endothelial axes in one run. For discovery panels that include IL-1β, IL-6, IL-18, TNF-α, and CRP, services like the Luminex cytokine detection service support customizable panels under RUO conditions.
Singleplex Assays for Targeted Inflammation Studies
Singleplex assays (e.g., ELISA, ultrasensitive modalities for low-abundance cytokines, and hs-CRP) are well-suited for targeted validation, cross-study comparability, or when analytical specificity is paramount.
Serum vs Plasma: Which is Better for Inflammation Biomarkers in Cardiovascular Research?
Matrix choice influences detectability and stability. Low-abundance inflammasome cytokines (IL‑1β/IL‑18) often benefit from EDTA plasma to reduce ex vivo release; CRP is typically robust in serum. Peer-reviewed guidance emphasizes predefining matrix/anticoagulant, processing within a few hours, and standardizing freeze–thaw limits for reliable cytokine reads. For matrix optimization and SOP-aligned workflows, see the Serum & plasma cytokine assay. When building a targeted panel for chronic atherosclerosis, a customizable approach like the Cytokine panel service can align biomarkers with matrix and volume constraints.
Platform Trade-offs at a Glance
Below is a quick side-by-side table to guide platform selection. Values are indicative; confirm per kit and matrix with fit-for-purpose validation.
| Platform | Typical sensitivity (LOD) | Dynamic range | Multiplex capacity | Typical sample volume |
|---|---|---|---|---|
| ELISA (singleplex) | pg/mL | 2–3 logs | 1 | 50–100 µL |
| Luminex xMAP | low pg/mL (analyte-dependent) | 3–4 logs | 50–100+ | 25–50 µL |
| MSD (ECL/S-PLEX) | pg to fg/mL | 3–5 logs | 10–50 | ≥25 µL |
| Simoa (ultrasensitive) | ~fg/mL | assay-dependent | Low (≤10) | Low (assay-dependent) |
| Olink (PEA) | low pg to sub‑pg/mL (panel-defined) | panel-defined | ~48 per panel | 2–10 µL |
For pre-analytical variables that affect cytokine detection (matrix choice, processing windows, freeze–thaw tolerance), comprehensive reviews in Cytokine (2021) and core-lab SOP resources outline practical parameters and their impact. For platform capabilities and sensitivity discussion, technology overviews from peer-reviewed methods articles and manufacturer technical summaries provide context for expected LODs and dynamic ranges.
Best Practices for Handling and Interpreting Inflammation Biomarker Data
Sample Collection and Storage Best Practices
Predefine matrix and anticoagulant (often EDTA plasma for low-abundance cytokines) and keep them consistent across the study. Process promptly—ideally within four hours—then aliquot to minimize future freeze–thaw and store at −80 °C. Limit freeze–thaw cycles (target ≤2–3), document deviations, and use matched cycles across comparative groups.
Data Interpretation Guidelines for Inflammation Biomarkers
Use research-context reference distributions rather than clinical thresholds, and track within-subject deltas across visits. Report LOD/LOQ, intra/inter-assay %CV, spike-recovery, and parallelism outcomes. Handle <LOD values via prespecified rules (e.g., left-censoring or justified imputation). Interpret in pathways: pair IL‑1β/IL‑18 for inflammasome activity; pair IL‑6/CRP for systemic load; consider TNF‑α with endothelial readouts when available.
FAQ
What are the main inflammation biomarkers in cardiovascular disease research?
IL-1β, IL-6, IL-18, TNF-α, and CRP cover the inflammasome, systemic acute-phase, and endothelial activation axes used in atherosclerosis and plaque vulnerability research (RUO).
When is IL-6 most relevant in cardiovascular research?
IL-6 is most informative for longitudinal risk tracking and for connecting local vascular inflammation to systemic response; pairing it with CRP strengthens systemic-axis assessment, as supported by multi-cohort analyses.
How do I choose the right biomarker for my cardiovascular disease study?
Align markers to the study question: use IL-1β and IL-18 to probe inflammasome-linked plaque vulnerability; use IL-6 and CRP for long-term risk and cohort enrichment; add TNF-α to capture endothelial activation dynamics.
How do serum and plasma differ for inflammation biomarker testing?
Both are used in RUO research. Plasma (often EDTA) can reduce ex vivo cytokine release and favors low-abundance targets (IL‑1β, IL‑18). Serum is generally robust for CRP. Keep matrix consistent across all time points.
What is the advantage of using multiplex assays for inflammation biomarkers?
A multiplex cytokine assay for cardiovascular biomarkers measures several targets from small volumes in one run, improving pathway coverage and conserving precious samples; confirm key findings with singleplex as needed.
References:
- Toldo, Stefano, et al. "The NLRP3 inflammasome and the IL-1 pathway in atherosclerosis." Circulation Research 122.12 (2018): 1722–1740. https://doi.org/10.1161/CIRCRESAHA.118.311362
- Tanaka, Toshio, Masashi Narazaki, and Tadamitsu Kishimoto. "Interleukin-6 in inflammation, immunity, and disease." Cold Spring Harbor Perspectives in Biology 6.10 (2014): a016295. https://doi.org/10.1101/cshperspect.a016295
- Batra, Gorav, et al. "Interleukin 6 and cardiovascular outcomes in patients with chronic kidney disease and chronic coronary syndrome." JAMA Cardiology 6.12 (2021): 1440–1445. https://doi.org/10.1001/jamacardio.2021.3079